|
Hepatic vascular hereditary malformations in
Westies, Scotties, Dandies, and Cairn terriers
Extrahepatic Portosystemic Shunt and Primary
Portal Hypoplasia Without Hypertension are the two most common
congenital hepatic disorders in these breeds .
Both diseases can coexist in the same dog.
According to Dr Center, both
malformations share the same genetic origin.
Primary portal hypoplasia without hypertension
may be 15 to 30 times more frequent than extrahepatic shunt in
predisposed breeds, but is usually less serious and remains often
undiagnosed.
|
SYMPTOMS
They usually appear in the first two years of life
(severe cases appear earlier, sometimes at weaning, but mild
cases can remain asymptomatic throughout the dog's life).
Up to 10-20% of dogs affected by a liver shunt are asymptomatic.
Symptoms are those with hepatic insufficiency, since the badly
irrigated liver cannot fulfill its role in detoxifying the
blood, or in producing proteins.
- Growth retardation, underweight
- Capricious appetite
- Gastrointestinal symptoms (diarrhea, vomiting)
- Behavioral and neurological symptoms (related to hepatic
encephalopathy and hypoglycemia, fatigue, prostration and
alternating agitation, aggression, vocalization, seizures,
tremors, coma)
- Increased drinking and urine
- Urinary symptoms related to urinary stones (kidney and
bladder)
Females are slightly more often affected because the
porto-azygos shunt (one particular type of extrahepatic shunt)
affects twice as many females than males.
|
|
Differences between the two anomalies:
The
shunt is a blood vessel that bypasses the liver, which produces
liver failure. Its gravity is proportional to the size and
position of the vessel (the porto-cava shunts are more frequent
and severe as the porto-azygos shunts)
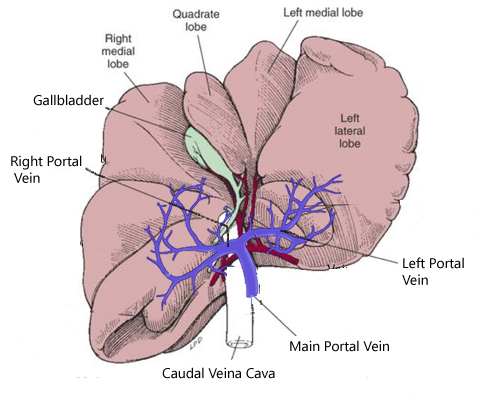
Primary portal hypoplasia without hypertension
affects portal vessels that supply the different liver lobes and
produces more or less marked effects, depends on the hepatic
lobes touched, leading to liver failure whose gravity is
proportional to the number of affected lobes.
This is a primary decrease in blood flow through the portal
vein, without atresia nor hypertension.
Hepatic vascularisation
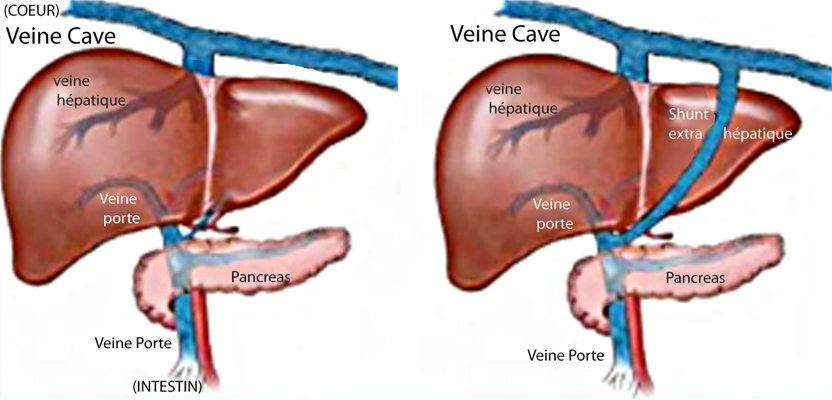
Normal hepatic vessels Extra-hepatic
Shunt ( porto-caval )
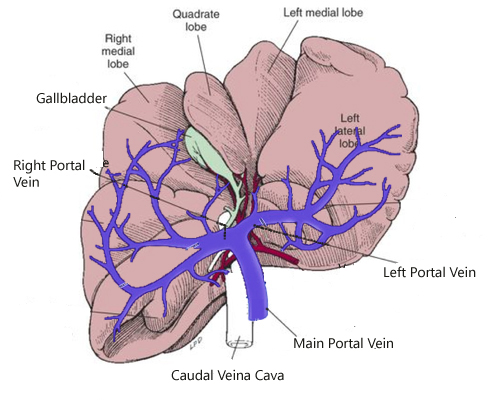 
NORMAL PORTAL
VEINS
HYPOPLASTIC PORTAL VEINS |
DIAGNOSTIC :
- Laboratory diagnosis of liver failure:
Determination of serum FASTING BILE ACID and POSTPRANDIAL (2:00
after a meal containing fat)
. Bile acids after 12 hours fasting are normally below 10
umol / l
This value is sometimes normal after prolonged fasting.
It is often normal for portal hypoplasia, and higher for shunts.
. Postprandial bile acids are normally below 30 umol / l
This value is always increased with hepatic vascular diseases
- Definitive diagnosis of a liver shunt extravascular:
-Ultrasound Fasting (first-line exam)
-IRM, Scintigraphy, portography, or Angio-Scan that has become
the test of choice, able to confirm a shunt and locate it if
ultrasound does not.
- Definitive diagnosis of primary portal hypoplasia:
It needs to eliminate the hypothesis
of a shunt first,
then biopsies on several hepatic lobes (at least 3).
|
|
Clinical and biological differences
between the two congenital vascular defects
The symptoms of liver shunt are generally more pronounced than
those of primary portal hypoplasia
The modified biological analyzes are in favor of a liver shunt:
- Microcytosis (erythrocytes)
- Low levels of serum urea, creatinine and cholesterol
- Moderate hypoproteinemia and hypoalbuminemia
- Hypoglycemia (fickle)
- Low level of serum protein C, often less than 70%
(the lower the C protein is, the severest is the shunt) |
|
TREATMENT
- Medical treatment of liver failure
syndrome (Antibiotics, lactulose, enemas, antiemetics, dietary
measures) and possible urinary complications (in case of urinary
stones)
This treatment is sufficient in many cases, especially in mild
symptomatic cases.
- Surgical treatment
It is conceivable in cases with obvious symptoms
. Ligature of the extrahepatic shunt.
According to the Dutch club's Cairn, 85% of liver shunt dogs
were operated on at the University of Utrecht at the age of 3-4
months and successfully, at an approximate cost 1000 €.
. Lepatic lobectomy during portal hypoplasia.
This surgery is much more delicate and rarely implemented
because the dogs affected with primary portal hypoplasia without
hypertension can usually be managed medically.
DIETARY MEASURES
Protein should be limited but high quality. The
best protein sources in this case are dairy products and soy.
Red meat, fish and giblets should be avoided.
Probiotics are recommended (some yogurts)
Special dietary foods for liver insufficiency exist and are
indicated.
|
|
GENETIC :
Dr. Center conducts research at Cornell University
(USA) to identify the genetic causes for these two diseases.
She concluded that a possible polygenic inheritance and maybe
the involvement of an autosomal dominant gene with incomplete
penetrance and variable expressivity.
In Europe, it is in Nederland that Pr. Van Steenbeek
and his team are conducting similar research on extrahepatic
shunt. He concluded with polygenic inheritance and the likely
involvement of two different genes.
Blood samples of the affected puppies are welcome at Utrecht
University
|
|
PUPPIES SCREENING :
It is essential to test the puppies having a weight
delays or other symptoms.
A simple determination of postprandial bile acids is sufficient
according to Dr Center.
The rate is generally :
greater than 70 umol/l in the case of
shunt
and less than 70 umol/l in the case
of primary portal hypoplasia.
A rate higher than 100 signs almost
certainly a shunt.
It should be done in all young West/Cairn/Scott in the first
year (the earliest possible) in order:
- To remove from the reproduction affected dogs.
In practice this means that young whose bile acids rates are
abnormal should be removed from the reproduction, even if it has
no associated symptoms.
- To quickly know the hepatic status of individuals. It is
important not to be in the situation later in their lives, to
have to differentiate between a liver disease present at birth
to an acquired liver disease, which would require multiple
invasive and expensive examinations.
In practice, breeders can screen puppies from 6-8 weeks (when
the puppy eats solid food) before they leave to ensure to the
new owner/buyer of the puppy that he is free of any vascular
congenital hepatic anomaly.
For the test to be valid and incontestable, the puppy should be
perfectly dewormed and identified beforehand, he should not
suffer from another disease at the time of sampling.
The test is cheap (16 euros per sample in France) and fast
(results the day of reception of the sample). It allows the
breeder to protect inexpensively from a sale of a puppy at risk
of developing an inherited disease in his youth.
The bile acids test is part of the 8 basic health checks
recommended by the Cairn Terrier Club of America before any
reproduction.
|
|
The RALIE
(French breed club for Irish Wolfhound and Deerhound) and liver
shunt
(RALIE website excerpt)
"Since 1 January 2009, the club has set up a program for
breeders who agree to follow the "Health + Standard" protocol
recommended by the club.
These breeders will have their litters published in the "Litters
A" part of the website.
4 points are required in this program:
1-Genetic identification of breeding animals;
2- Official Screening of DilatedCardioMyopathy before the mating
(with result clear);
3-Screening puppies for portosystemic shunt they live the
breeder;
4. etc. " |
|
Extract from the Nederland Cairn
Terrier Club (website)
"Conclusions :
For a large
number of years, the Netherlands’ Cairn Terrier Club has pursued
an intensive policy with respect to the assessment of liver
shunt and to reduce the percentage of shunt sufferers in the
breed. An increasing percentage of puppies is being tested.
Meanwhile, 90% of the breeders, who are members of the NCTC,
have their puppies tested. From 1991, more than 6000 puppies
have been tested. The percentage of puppies diagnosed with a
shunt has decreased from 3% until below 1% at the moment.
Despite all measures taken and all attention paid to the
problem, every now and then a puppy is born with a shunt,
although from the combination of parent animals no higher risk
could be expected. Ultimately, the results of the DNA research
at Utrecht University will enable to guide breeding programmes
further. In conclusion, we can put that the problem of liver
shunt in Cairn Terrier breeding has been handled energetically.
Much has been achieved in a limited number of years thanks to
the major cooperation from breeders, the policy of the breed
club, and the outstanding cooperation between Utrecht University
and the Netherlands’ Cairn Terrier Club. In future, we need to
be vigilant. Finalisation of the DNA research into shunts in
Cairn Terriers should be the next important step forward."
Details of the screenings from 1990
to 2012:
From 1990 to 1993 the affected cairn
puppies were 2.48%,
From 1994 to 2001 they were 0.96%.
Now the Cairn terrier puppies affected
by a congenital liver shunt are less than 0.5% among the tested
litters.
|
year |
puppies tested |
puppies no tested |
shunts |
|
2001 |
580 |
65 |
4 |
|
2002 |
604 |
87 |
1 |
|
2003 |
596 |
92 |
2 |
|
2004 |
Not published |
|
|
|
2005 |
563 |
74 |
1 |
|
2006 |
454 |
49 |
1 |
|
2007 |
428 |
28 |
5 |
|
2008 |
386 |
38 |
1 |
|
2009 |
341 |
8 |
3 |
|
2010 |
360 |
7 |
0 |
|
2011 |
325 |
5 |
1 |
|
2012 |
393 |
0 |
3 |
|
Bibliography:
Dr Van Steenbeek and coll /Université
d’Utrecht, ND (Distribution of extrahepatic congenital portosystemic
shunt morphology in predisposed breeds)
Dr Shanon Center /Cornell University Ithaca,
New York, USA (article du Merck veterinary Manual = Portosystemic
Vascular Malformations in Small Animals)
Dr Avril Hamel Jolette and Dr Lyanne Fifle/centre
vétérinaire DMV de Montréal Canada (Anomalies vasculaires hépatiques
congénitales)
Dr Karen M.
Tobias/ University of Tennessee, Knoxville,USA (Understanding
common liver disorders in Yorkshire Terriers & other toy breeds (2013))
|